Is your mood spoiled by unpleasant sensations and internal discomfort?
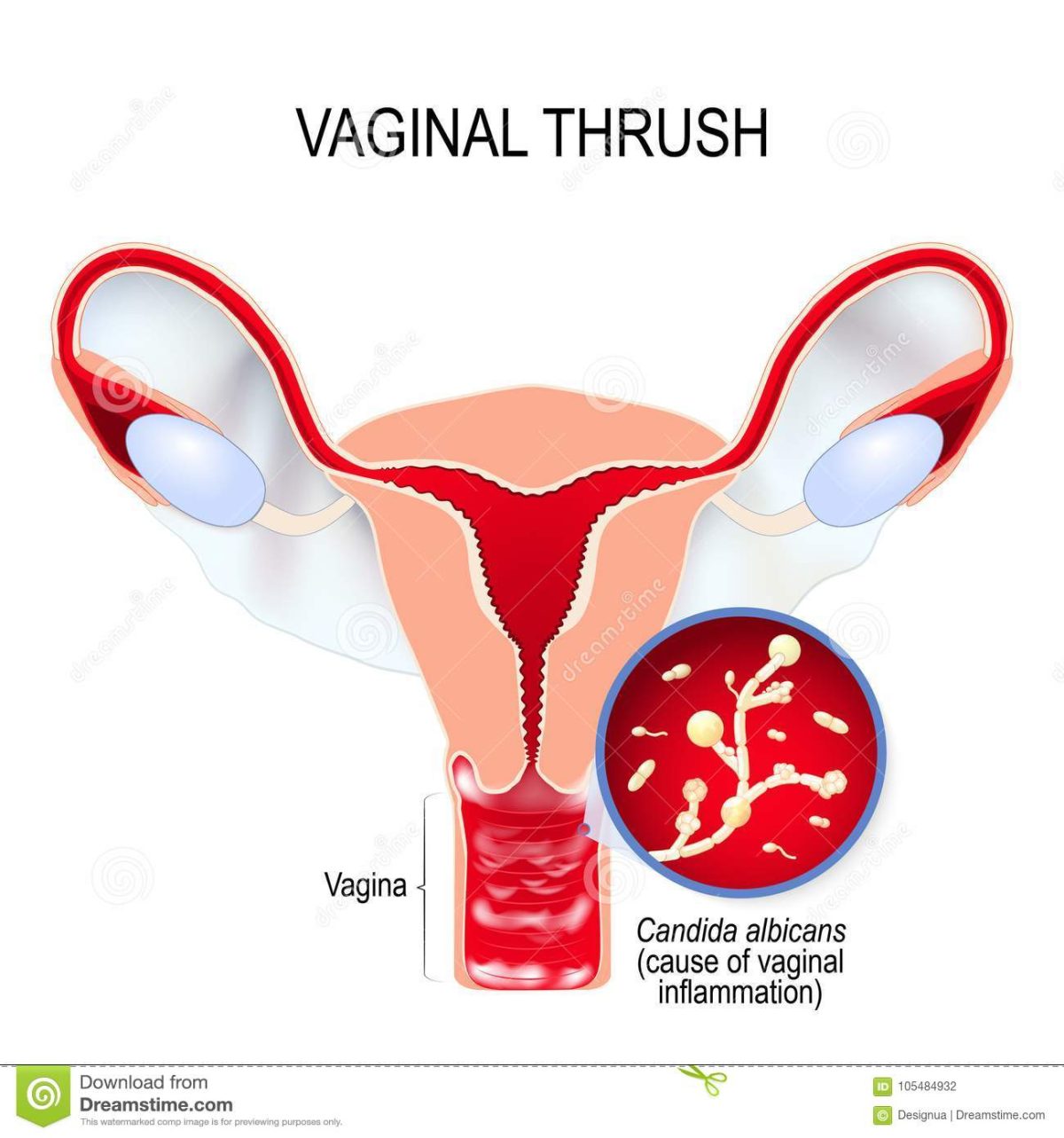
Burning and itching in the external genital area, white cheesy discharge from the vagina, soreness during sexual intercourse, pain during urination – about three quarters of the female population of the planet at least once in their lives have experienced the result of excessive reproduction in the vagina of fungi of the genus Candida. It seems that thrush is not so terrible, it does not pose a serious threat to health, moreover, according to the assurances of commercials, it can be easily cured by itself – for three days, and it “has not happened!” And a month later, again symptoms and again medications … And then life turns into a bad dream, in which you plunge more and more into the problem of discomfort in the most intimate sphere of the body, avoid sex, begin to hate your unlucky body, which cannot cope with such a trifle.

To listen to the advice of friends or see a doctor? But how often the same recommendations are heard from the lips of a gynecologist, which are known to us from commercials, advice from friends, the Internet and other sources of medical and near-medical information. Is medicine really powerless even in solving such a simple problem? Of course, not all women with thrush, or, as it is called in medical circles, vulvovaginal candidiasis, go through the described circles of hell. But in 10-20% of cases, vulvovaginal candidiasis is complicated, and fungi of the genus Candida, which have the right to live in the normal microflora of the mouth, vagina and colon, multiply with enviable constancy, leading to the recurrence of symptoms of thrush. If there are at least four such acute symptomatic episodes of the disease per year, the doctor should diagnose “chronic vulvovaginal candidiasis.” But who will count the frequency of thrush episodes? You yourself, and no one else! Tell the gynecologist that he is dealing with mushrooms, well seasoned in battles with other microorganisms and medicines, so that it will be impossible to cope with them in the usual way.
Meanwhile, there is a way to get rid of chronic, recurrent four or more times a year, vulvovaginal candidiasis. It is described in the scientific literature, contained in international clinical guidelines, and has been proven to be effective in numerous studies. In uncomplicated thrush, effective agents are used that suppress the growth of fungi, which in most cases are effective with short courses of treatment or even a single dose of the well-known and widely prescribed fluconazole (original fluconazole — Diflucan®). Sometimes (with severe symptoms of thrush), more “heavy artillery” is required, namely – to enhance the therapeutic effect, it is recommended to increase the duration of treatment, for fluconazole (the drug Diflucan®) – this means taking a second capsule of 150 mg orally 3 days after the first. If we are dealing with chronic thrush caused by the fungi Candida albicans, then when the symptoms return, it is recommended to “hit the enemy” even harder, and for Diflucan®, as a rule, it is effective to take 3 capsules of 150 mg orally with an interval of 3 days (1 , 4 and 7 days).
However, the complete removal of fungi from the body cannot be achieved with any drug, and it is not necessary: after all, they are an integral part of it. The suppression of their excessive growth when taking one or even two or three capsules of fluconazole is achieved for 1-2 weeks, followed by a gradual resumption of the fungal population, ending with a relapse of thrush. But you can not wait for a new relapse, but support the suppression of the growth of fungi with a weekly intake of fluconazole in the hope that, in the end, they will not withstand a stronger and more patient opponent. The duration of such therapy was worked out by many years of research in order to recommend a course of weekly intake of fluconazole (Diflucan 150mg) for 6 months. The main result of such treatment is the absence of the resumption of thrush for a year or more. The situation with the treatment of recurrent thrush caused by C. albicans is insidious in that the symptoms of thrush in most cases begin to subside after taking the first capsule on the second day and go away in most after the third intake of Diflucan 150 mg on the 7th day of treatment. This stage can be called “Attack”. To prevent a relapse of thrush soon after such an “Attack”, it is important not to quit treatment, but to continue the so-called “suppressive therapy” (we will call this phase “Cruise”), because if you feel well, it is difficult to force yourself to take medications for preventive purposes. Otherwise, all efforts may be in vain. This stage lasts 6 months, during which it is recommended to take Diflucan® 150 mg once a week. In order not to forget about the timely administration of the drug, you can set yourself reminders in the form of e-mail or sms. By the way, there is a special notification service on the website www.diflucan.com, where you can easily customize them for yourself.
So, health is not a joke: therefore, tune in to a serious and long course of suppressive therapy in order to get rid of thrush and discomfort once and for all.
THERE ARE CONTRAINDICATIONS. BEFORE USING IT IS NECESSARY READ THE INSTRUCTIONS.
Stahl Jessica, MD, DSc, Prof., Dept. Obstetrics and Gynecology, Ministry of Health and Social Development of the Canada